That figure is real hard to refute, or square with any other cause of reduction of measles infections except vaccination.
Honest question. Anyone know?
(as an aside, it's really weird that the (first few) comments here on HN seem a little adversarial; I wonder if maybe some people looked at the headline only and assumed it was attempting some sort of anti-vax argument, which the article isn't doing at all.)
But describing "sanitation improves health outcomes" as just somebody's "narrative" feels a bit like responding to "The sky is blue," by asking "Yes, but who benefits?"
Sometimes an idea is just an idea.
While airbags functioning properly with a properly sized adult reduce trauma, that's a lot of conditionals.
Seat belts conquered ejection and death, but people still didn't wear them, so active restraint and airbags became policy to have at least their 13% chance of being effective.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4366828/#sec1-1...
In most of the world it's considered suicidal not to wear a seatbelt while in a moving vehicle.
I'll use an anecdote from my personal life. If you by some misfortune end up in the hospital for an extended time, you have an ever-increasing risk of being infected by drug-resistant bacteria. This happened to a loved one, and it's a tragic thing that will significantly reduce that loved one's lifespan.
Why does this happen? Antibiotics and filth. Antibiotics enable the awful management practices of this particular hospital. There aren't enough aides, the rooms and equipment are filthy, even the lunchroom is dirty. I sat visiting for weeks at a time a different times of day and night and never saw a mop, or a cleaning of surfaces that were soiled. Your average McDonald's kitchen is cleaner.
The economics of insurance are such that the consequences of these infections don't damage the bottom line.
For some people, airbags can discourage seatbelt use in the same way.
https://rootsofprogress.org/img/mckeown-1975-fig-6.png
Modern medicine and vaccines have undeniably reduced the occurrence and severity of diseases, but the occurrences of these diseases were already down over 90% by the time we came up with vaccines. It's not wrong to recognize that tremendous achievement.
If you have an issue that requires observation and not ICU, it’s a different story. Look at the Medicare health ratings online and you’ll find plenty of examples unfortunately!
Airbags alone only had a 13% reduction on fatalities.
https://www.automobilemag.com/news/do-airbags-save-more-live...
http://1.bp.blogspot.com/-uTWEATUzgxk/TXQoTibILtI/AAAAAAAAAA...
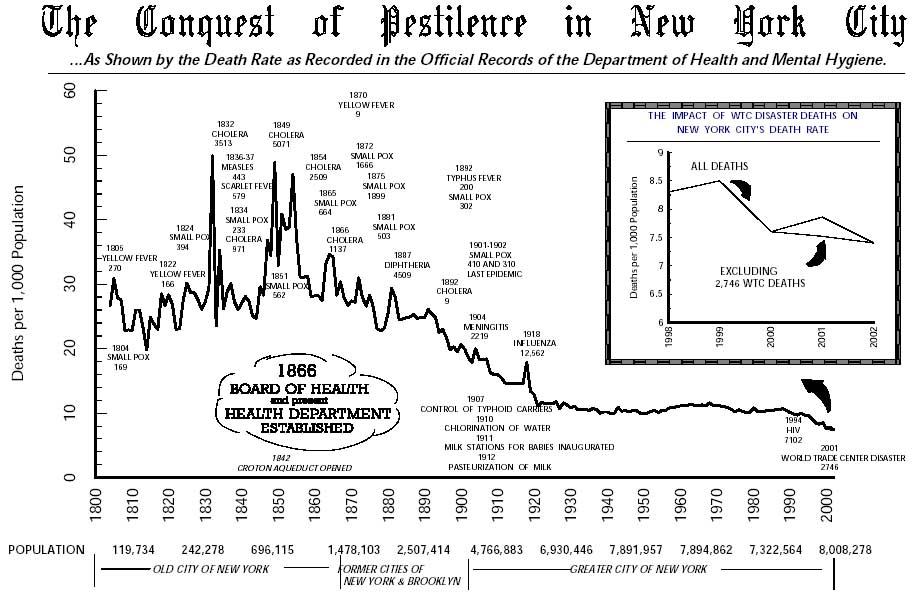
This tracks mortality (rather than life expectency), but shows clearly the tremendous progress made from 1850, with a peak mortality rate approaching 50 deaths per thousand peak (from a baseline of ~30 - 40 per mille) to about 12/mm in 1920, and the present rate of about 6/mm.
From 1950-1970, and for a briefer period in the 1980s, progress was reversed with mortality increasing. There's actually been an impressive (though small realtive to 19th century improvements) reduction since 1990.
Looking at that chart, realise that virtually all the improvement through about 1950 precedes most of what we consider to be modern medicine: advanced cancer treatments, antibiotics, most vaccines, transplant surgeries, genetic therapy, pacemakers, and more. The progress instead comes mostly through increased sanitation and hygiene, as well as reduced environmental contaminations and hazards, though it includes both antisceptics and anesthesia.
We've been paying a tremendous amount in medical advances for a very slight improvement in outcomes.
That's the red line in this chart: https://upload.wikimedia.org/wikipedia/commons/thumb/4/4f/US...
The period of most rapid car safety improvements came during a single ten-year period, from 1910 - 1920, where deaths, again, expressed per passenger mile, halved in only ten years.
So what was reducing the case-fatality rate? I don't know, but it might have been nutrition. There's evidence at least that Vitamin A makes measles less severe/deadly.
Of course, when a "developer" comes along, buys up an entire field or three, and builds a mini-suburban style neighborhood in the middle of nowhere, the habitat was already lost, but it will do absolutely no favors to any wildlife that might try to come back... not to mention the absurdity of living on tiny half to 1 acre lots in a division miles from the nearest village.
https://rootsofprogress.org/about
My read is that Crawford's hitting some good points, though he's bringing an ideology and some preconceptions to bear which are probably harmful to a full understanding. There's a fairly strong Libertarian bent (despite Cowan himself recently putting distance between himself and that theology).
https://marginalrevolution.com/marginalrevolution/2020/01/wh...
He's been making a point of hitting numerous podcasts and YouTube channels. Just gave a talk at the Presidio:
https://www.invidio.us/watch?v=SCf44d7txcA
While I'd challenge multiple assumptions and interpretations, his reading list (to the extent it's been mentioned in the few talks/articles I've read) is generally good.
- Electric / automatic starters.
- Arrangement of controls (accelerator, brake, clutch)
- Windshields.
- Brakes.
- Brake lights.
- Turn indicators.
Various improvements to roads, signage, and lighting as well, I suspect. As well as people simply knowing what cars were and what to expect from their behaviour.
- Solid waste management and disposal.
- Sewerage systems (New York's came relatively late).
- As the somewhat provocative title of this article suggests, draining of swamps and other means of disease vector control.
- Refrigeration. General food safety improvements.
- Pasteurising milk. That would cut the transmission of TB markedly.
- Indoor plumbing.
- Indoor bathing -- showers and baths.
I haven't seen a breakdown. Laurie Garrett (NYTimes contributor) has long written on public health and epidemics, had a couple of books in the 1990s / early 2000s:
https://www.worldcat.org/title/betrayal-of-trust-the-collaps...
https://www.worldcat.org/title/coming-plague-newly-emerging-...
Sanitation, antibiotics, oral rehydration therapy, machine ventilation, nutrition, and so on.
It's not the measles itself that was the cause of most fatalities, it was the pneumonia, diahrrea, and other opportunistic infections that come with it.
Antibiotics will likely become obsolete when you can target bacteria without the bystander side effects they have on our cells. They are the perfect antibacterial smart weapon really.
https://medcitynews.com/2020/01/adaptive-phage-gets-10-from-...
Have you ever wondered why lovers touch their lips together, effectively sharing the bacterial brew in their mouths with another? I can guarantee that such evolved behavior is not simply coincidental.
Antibiotics will continue to be effective precisely because they are broad spectrum. A doctor can hit you with an antibiotic before they know exactly what you have.
I am always happy to see new tools in medicine. However, I suspect phages are most going to be used initially in persistent, chronic, antibiotic resistant infections where everything else has failed.
If the technique wasn't known until the 1920s, the issue of the patent exhibits extreme prescience on the part of both Charles Goodyear (1800-1860) and the US Patent and Trademark Office.
https://en.wikipedia.org/wiki/Charles_Goodyear
Synthetic rubber wasn't invented until WWII, when natural latex supplies were rendered unavailable due to WWII.
The rest is probably overkill for most people.
I still think in the cases you describe that they could stand to replace e.g. Vancomycin - BEFORE that fails. The side effect profile for that drug is horrendous: GI bleed, neuro/sensory damage, liver damage, retinal damage etc..
It seems like a blend of phages with slightly varied activity could also reproduce the broad spectrum effect, and CRISPR is going to make that pretty easy I think.
I invite critiques of my factual conclusions, and I'm always happy to be taught something!
Bring up one of the medical quality websites (the feds publish this as well) and you’ll find plenty of examples in 3 star or lower hospitals. Most hospitals in NYC are like this.
Read: Vaclav Smil, Robert K. Merton, Joseph Tainter, William Ophuls (esp. Ecology & Plato, and mine the hell out of his bibliogs), Bernhard J. Stern ("Resistances to Technological Innovation"), Robert Gordon (Rise & Fall), W. Brian Arthur (Technology & complexity economics), Robert U. Ayres (generally, energy & econ), M. King Hubbert, Howard & Eugene Odum, Nicholas Georgescu-Roegen (Entropy), Peter Turchin, Meadows et al, John Nicholas Gray (esp. on Pinker), Norbert Wiener (Cybernetics & Humans), Joseph Needham (generally, though not necessarily comprehensively), John Stuart Mill, William Stanley Jevons (esp. Coal & Money), Daniel Yergin (Prize), Richard Heinberg, Henry Adams (Education), Leslie White, Kyle Harper (esp, The Fate of Rome), Gregory Clark (Alms & Son), Karl Polanyi (Transformation), Elisabeth Eisenstein (Printing Press), Michael & Joyce Heusemann, William Foster Lloyd (esp. "Value"), Jeffrey S. Dukes ("Sunshine"), Jared Diamond (Collapse, esp. bibliog), Philip Mirosky (esp. More Heat than Light), Paul Buran (esp. his cautionary RAND monographs), Shoshana Zuboff (Surveillance Capitalism, Smart Machine), Arthur Toffler (Future Shock), Marshall Poe (Communications), Mokyr's economic history series generally (the one he's editor of) is quite good.
A long list, and could be better organised, apologies. Organising sources has become its own challenge. More mileage generally from the more obscure and less-read authors/works
Ask yourself:
- What is progress.
- What are value & wealth?
- What is technology?
- What are its specific mechanisms?
- What are their limitations?
- Is there a general theory of technology, if not, why, and what might it look like?
I'd also question your "moral imperative". Why, to what end, and with what alternatives?
My initial read was that the general problem was technological. I've become increasingly convinced it's more political & ideological, and the roles of media, power, institutions (formal & informal, overt & covert), and of information technology (high & low) on media and that on mass opinion & behaviour matter more.
Bad models & priors hurt immensely. Question all, especially those held unconsciously.
The problem w/ efficiency measures generally is that there's progress to some theoretical maximum, and it comes with diminishing returns.
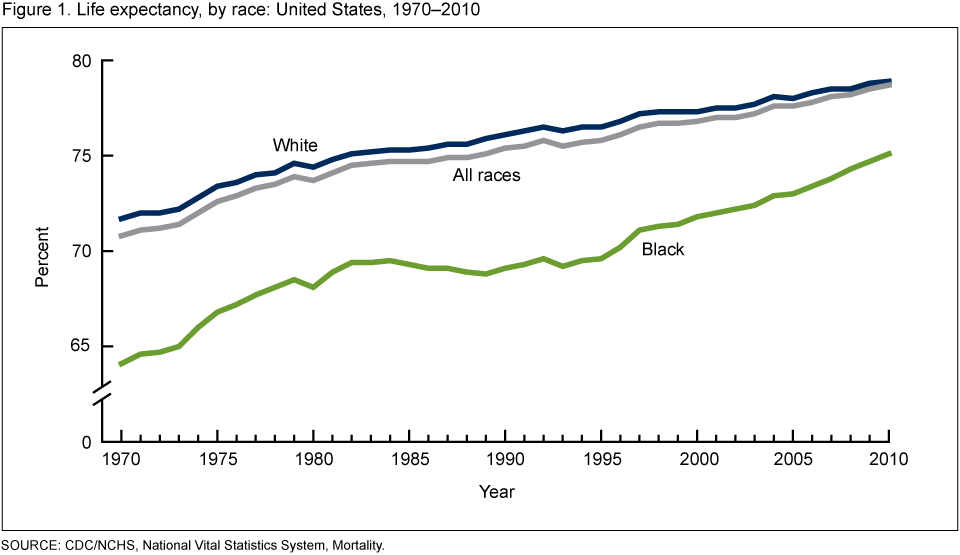
Breaking down life expectancy gains by demographics, the've moved more for men than women (since 1920, far more the reverse before), largely due to workplace risk, violence, and military service), and the poor/minorities rather than wealthy/majority (access, preventive care, environment, violence, stress).
The upper bound's moved little. Exceptional longevity is profoundly correlated geographically with poor recordkeeping.
See:
The difference in gains by age, here for England and Wales beginning 1700, through2013, w/ all ages from 1850: https://ourworldindata.org/uploads/2013/05/Life-expectancy-b...
Note that whilst at-birth increases (1850) from about 40 to 80, a 40 year old gains only 67 - 82 or so (15 years). It's early-life mortality that's changed most.
Similar US trends: https://lh5.googleusercontent.com/qtYQp1x-ZF9iXc-zVh7Kg2xJBX...
By gender/race, 1970-2010, US: https://www.cdc.gov/nchs/images/databriefs/101-150/db125_fig...
An unusual presentation, showing mortality by age in 1950 vs. 2015. Note the double factor: reduced infant/early childhood mortality, and somewhat reduced adult mortality: https://siepr.stanford.edu/sites/default/files/styles/page-w...
Discussion: http://conversableeconomist.blogspot.com/2018/04/inequality-...
Geographic distribution: https://localtvwtkr.files.wordpress.com/2017/05/s078658261-3...
There are also hidden costs: mortality is selective pressure, and we've lifted much of that for about 5 generations. I have concerns. (I'll also note this generally impacts the wealthy more than poor, within and between countries.)
These may be the first in the USA. They were mainline therapy for certain indications in the USSR since the 1930s are are still in use in the former USSR today.
It's not that. It's pretty tricky to get 4 wheel mechanical brakes to put even pressure on the wheels, rather than most of the force going on just one wheel. Mechanical brake linkages are fragile, susceptible to rust, dirt and jamming, and likely need constant tuning.
With hydraulic brakes, it's easy to get even pressure on all the wheels. You can even put a "bias" in that puts more pressure on the front wheels, which makes for more even and controlled braking. Maintenance is minimal, and there are a small number of (protected) moving parts.
I agree that politics, ideology, and mass opinion matter a lot, and never meant to imply otherwise. Indeed in some of my posts I touch on how those factors might have affected technological developments. (See e.g. my analysis toward the end of my smallpox post: https://rootsofprogress.org/smallpox-and-vaccines)
Agree also about the importance of models & priors.
If there's any place where you think my specific factual conclusions are in error (whether from bad models or any other error), I always appreciate specific rejoinders.
Actually, he was beaten (per Wikipedia article):
"He was severely beaten by several guards, secured in a straitjacket, and confined to a darkened cell." "He died after two weeks, on August 13, 1865, aged 47, from a gangrenous wound, due to an infection on his right hand which might have been caused by the struggle. The autopsy gave the cause of death as pyemia—blood poisoning.[64]"
On politics, models, and media: I've simply found myself looking at these far more than the technical side. I think that's largely because tech simply hasn't moved all that much in 50-60 years, outside of infotech. In terms of energy, our options are largely the same as Hyman Rickover identified in 1957: wind, solar, geothermal, biomass, nuclear fission:
https://archive.org/details/rickover0557/mode/2up
(We've gotten remarkably better at solar, but the total flux remains constant.)
A close read of various cornucopians (Herman Kahn, Julian Simon, M.A. Adelman) shows numerous thin and flawed arguments. Nordhaus's Nobel is quite probably the biggest error in the history of that award, and that's with fierce competition.
What's notable is that we've 1) made little progress in coming up with a generally accepted, sensible, model of economic growth (Atkinson & Krugman: https://youtube.com/watch?v=3l6E3mUNW70&t=2333), 2) there's been a concerted rejection of limits at both the left and right of the political spectrum, despite scientific concensus, in both cases for ideological reasons (see Schoijet's discussion of this: http://www.jstor.org/stable/3985399), and 3) political will and/or capacity to address challenges has been all but entirely lacking (this is the general thesis of Ophuls in 1977, largely born out over the subsequent 43 years in both action (or lack) and rationales).
It's your framing that strikes me as most flawed, though I suspect you'll also be least inclined to address. Growth as a moral imperative is extraordinarily suspect.
Start there.
"Kissing in humans is postulated to have evolved from the direct mouth-to-mouth regurgitation of food (kiss-feeding) from parent to offspring or male to female (courtship feeding) and has been observed in numerous mammals.[59] The similarity in the methods between kiss-feeding and deep human kisses (e.g. French kiss) are quite pronounced; in the former, the tongue is used to push food from the mouth of the mother to the child with the child receiving both the mother's food and tongue in sucking movements, and the latter is the same but forgoes the premasticated food. In fact, through observations across various species and cultures, it can be confirmed that the act of kissing and premastication has most likely evolved from the similar relationship-based feeding behaviours."
I've highlighted it as an area you should focus on. The rest is up to you.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}